

Original
Progressive ageing of working population in a southern Spain reference hospital
Envejecimiento progresivo de la población trabajadora en un hospital de referencia del sur de España
Actual. Med. 2019; 104: (807): 92-97 DOI: 10.15568/am.2019.807.or03
Enviado: 10-06-2019
Revisado: 04-07-2019
Aceptado: 20-07-2019
ABSTRACT
The aim of this study was to describe the work population evolution of a southern Spain hospital along a decade (2006-2016), focusing in the predominant staff.
Methodology. A descriptive cross-sectional epidemiological study was undertaken to build up a population pyramid. The cut-off point was January 2017. The scope was the work force of a regional hospital with 5450 members, 1408 of which were nurses. One index was calculated to relate youth with the older population; and another one to look at femininity.
The results revealed an inverted pyramid-shaped, narrow-based and feminized asymmetric, demographic structure, and a progressive ageing after a decade. The femininity index was even higher for the nursing population. The working population over 50 years was greater than that below this age. There was a striking narrowing in the 51-55 age stretch, but only in female nurses.
We conclude that there is an ageing working population and a predominance of women in almost all age groups, especially in nurses. There is an imbalance that makes it necessary to plan health monitoring. In such a way that demographic studies would facilitate collective health monitoring by prioritising actions according to age and sex variables. The low percentages of young nurses, together with the fact the age of the retirement in the studied population is lower than the legal one, are facts which must draw the attention of Spanish managers to put in place realistic and efficient measures that promote the “active ageing” so often spoken of as well as others that facilitate the entry into the labour market of young workers.
Keywords: Labour demographics; population pyramid; retirement; nurses; health surveillance.
RESUMEN
El objetivo del estudio fue describir la evolución de la población laboral en un hospital de referencia del sur de España durante una década (2006-2016,) centrándose en la categoría laboral predominante: las enfermeras.
Para ello se realizó un estudio epidemiológico descriptivo de tipo trasversal, en forma de pirámide poblacional, cuyo punto de corte fue enero de 2017. El ámbito de estudio fue la población laboral de un hospital regional del sur de España con 5450 profesionales, de las que 1408 eran enfermeras. Se calcularon índices, uno para relacionar la población joven con la madura y otro de feminidad, comparándose con un informe previo de 2006.
Los resultados mostraron una estructura demográfica en forma de pirámide invertida, de base estrecha, y asimétrica. Con una población laboral envejecida y feminizada en casi todos los tramos de edad, siendo el índice de feminidad aún mayor para la población de enfermeras. La población laboral mayor de 50 años, superaba a la menor de dicha edad. Existía un estrechamiento llamativo en el tramo de 51 a 55 años, solo en las mujeres enfermeras, que interrumpía el incremento progresivo de la población laboral que le antecedía.
Concluimos que la población laboral estudiada ha envejecido progresivamente, con un predominio femenino mayoritario, especialmente en las enfermeras, apreciándose desajustes que obligan a analizar las causas y a planificar actuaciones. Los estudios demográficos pueden facilitar la vigilancia de la salud colectiva priorizando actuaciones según las variables edad y sexo. El escaso porcentaje de la fuerza laboral joven y el hecho de que la edad de la jubilación real del personal estudiado sea inferior a la legal debería llamar la atención de los gestores para aplicar medidas eficientes que promuevan el “envejecimiento activo”, así como otras medidas que faciliten la entrada de los jóvenes en el mercado de trabajo.
Palabras clave: Demografía laboral; pirámide de población; enfermeras, jubilación; vigilancia de la salud.
Leer Artículo Completo
INTRODUCTION
Demographic studies are usually prepared based on data from official regional (1), national (2), or transnational (3) statistics institutes, while the number of studies that show working population pyramid data are relatively few. The general data show that Europe is ageing (4). In Spain there are official statistics obtained from the municipal residents registers and the national census. The last census (2), carried out in 2011, showed that 25% of the population were aged over 50. The forecasts estimated an average age of between 45 and 59 for the working population during that decade (5).
Analysing the labour demographics of a place of work where large numbers of people are employed may be useful for gaining a picture of the contemporary labour structure and to observe its evolution, serving as a guide for hospitals of a similar size in developed countries. In the case of regional referral hospitals, the scope of influence encompasses the citizens of the province and the surrounding geographic area, catering for populations of over one million.
On the other hand, the legislation in place in Spain establishes that monitoring collective health must form part of the daily activities of prevention services (6). In addition to classic epidemiological studies (7), we can consider others such as demographic studies. It is interesting to ascertain how the labour force is distributed by age and sex, with special attention on the qualitatively predominant labour category, such as nursing.
There are hardly any demographic studies carried out in the labour environment in the scientific literature. The main objective of the study is to draw up a labour population pyramid of a referral hospital in the south of Spain in order to describe, analyse, share the predominance of nursing and observe its evolution over the last decade based on the hospital’s annual report.
METHODOLOGY
Design
For the demographic analysis of the labour population, a cross-cutting transversal epidemiological study was carried out.
Area of study
The area of study is the working population of a regional hospital in the south of Spain (European Union), and the period of study was January 2017.
Population and sample
The population study looked at all the employees of the referral hospital analysed, dependent on the Health Service of Andalusia, which at the time of the study consisted of a total of 5,450 employees, making it the largest employer in the province in which it is located. Of total hospital staff, the majority (52.3%) belong to the nursing division, 27.4% are non-healthcare staff and 20.3% belong to the medical division.
Criteria for inclusion and exclusion
The criterion for inclusion was a direct contractual relationship with the hospital, including personnel with temporary contracts at the time of the study. For the nursing population, both degree and diploma graduates were considered along with middle and senior managers. Neither matrons nor nursing assistants were included in the nursing population as they belong to another professional category. The criterion for exclusion was the absence a contract with the hospital due to being employed by an external company, such as cleaning staff.
Sources for collection of data
The population structure was compiled based on an anonymous database built from the transfer of data registered on winmedtra, the software used for workplace health exams, which included the entire working population of the hospital. The data for the analysis of the evolution of the working population were obtained from the 2006 annual report, prepared in the same regional hospital (8).
Data analysis
The total population and the nursing population were quantified using absolute and relative data and the age and sex variables using the Excel program of the Microsoft Office package, officially licensed through the University of Córdoba. Based on this data, tables were composed; one with the total population and another with the nursing population, dividing the staff by five-year age brackets from 25 to 65 along with the two extremes: 65. The graphics of the working population pyramid were comprised using the data from the tables. For the 65 age brackets, the Excel function COUNTIF was used for the “age” column using the 65 data so that only the data for those aged 24 or younger of 66 or over were included. In the rest of the age brackets, the Excel function COUNTIFS was used selecting the above data, and so on for each of the corresponding age brackets. To compile the nursing population table, the same Excel function was used but only for “A.T.S/D.U.E.” graduates. For the classification of staff by age and sex, in percentages, the function COUNTIFS was used for the “age” and “sex” columns in all sections.
For the purpose of relating the young and mature population an index was comprised where the numerator was made up of the number of employees under 30+100 and the total denominator of the 30 to 50 bracket. The femininity index and the average age of the population analysed was also calculated.
Ethical considerations
The study was developed within the framework of a research project titled “Interventions to promote active and healthy ageing in the workplace based on the model for action on working capacity” which meets with the express approval of the corresponding ethical committee. The database was anonymized to meet the relevant legislation (9), as part of a final year degree dissertation with shared authorship between the first two signatories of this article.
RESULTS
The average age of the hospital population when analysed in 2017 was 50.12, and that of the nursing staff was 49.78. The 2006 report showed an average age of 45 for all staff.
The index proposed to compare the young population with the adult population was 15.48% for the total population (313*100/2022), having been 9.86% in 2005 (313*100/3174).
Table 1 shows the distribution of the total working population of the hospital by age bracket, with absolute and relative data, differentiated by sex. Access for people aged over 50.
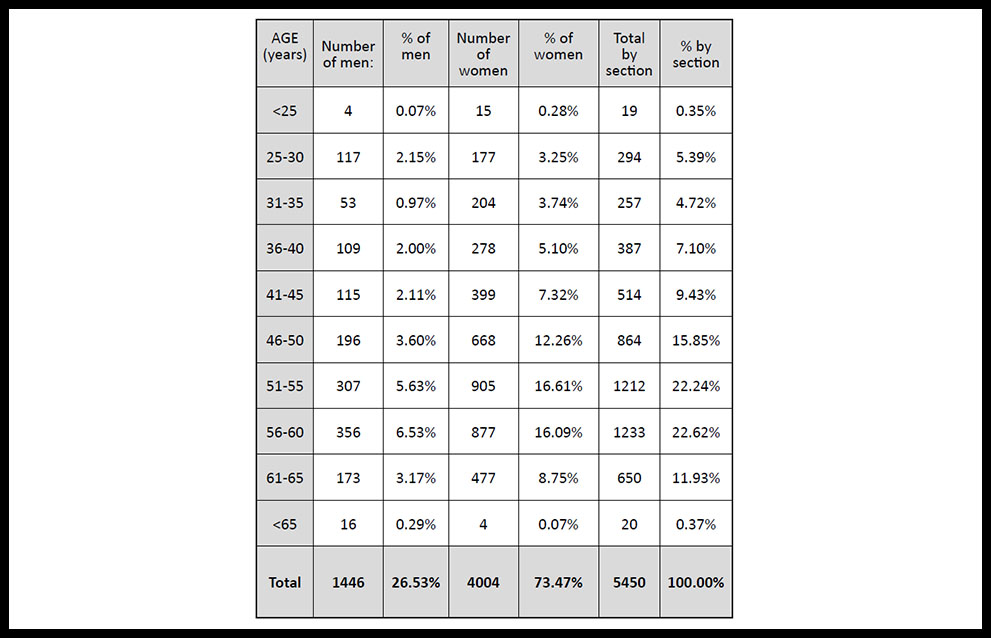
Table 1. Quantitative distribution of hospital staff by age bracket and sex.
The femininity index obtained for the total working population was 73.47% (4004*100/5450), having stood at 70.37% in the 2006 report (3549*100/5043).
In order to immediately visualize the structure of the total population of the hospital, we compile the corresponding pyramid (figure 1). We observe an asymmetric inverted pyramid with a narrow base, heavily female dominant in all age brackets, except for staff aged over 65 as there are no workers in this final extreme age bracket. The working populations of each bracket increases progressively only to fall from 60 on, except for men in the 25 to 30 bracket, which is higher than the 31 to 35 age bracket. The contracting of the extremes and the predominance of the age brackets between 51 and 60 are particularly noteworthy.
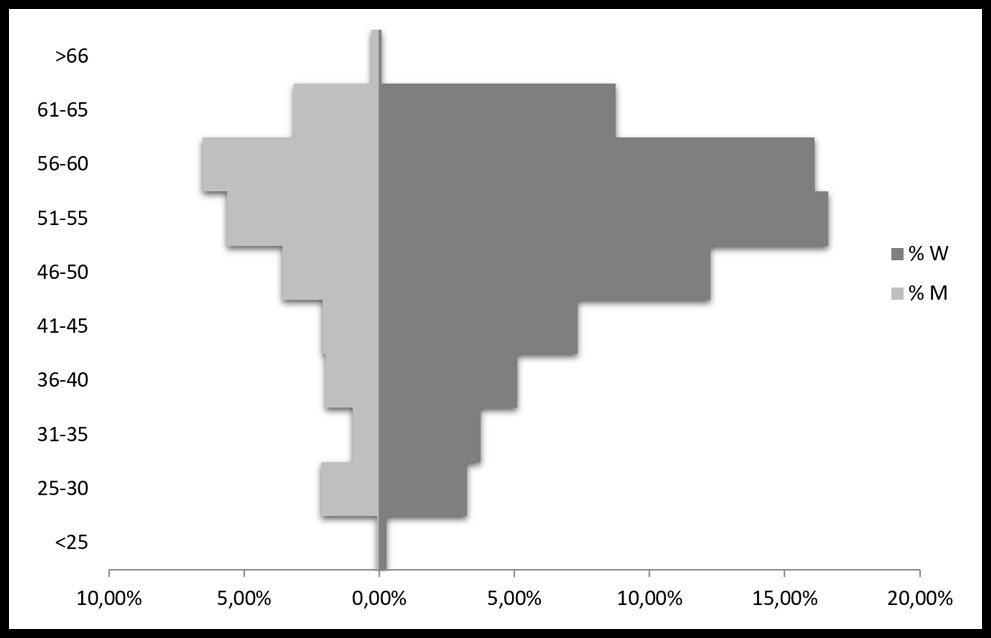
Figure 1. Population pyramid according to age and sex from a southern Spain regional hospital.
A total of 1,408 professionals from the 2017 study were nurses (1342 in the 2006 report). The femininity index for the working nursing population was 83.59% in 2017. This was higher than the 73.47% for the total hospital population. The index proposed to compare the young population with the adult population was 2.87% for nurses (20*100/696).
Table 2 offers the qualitative, absolute and percentage data by age bracket and sex for the hospital nurses in 2017.
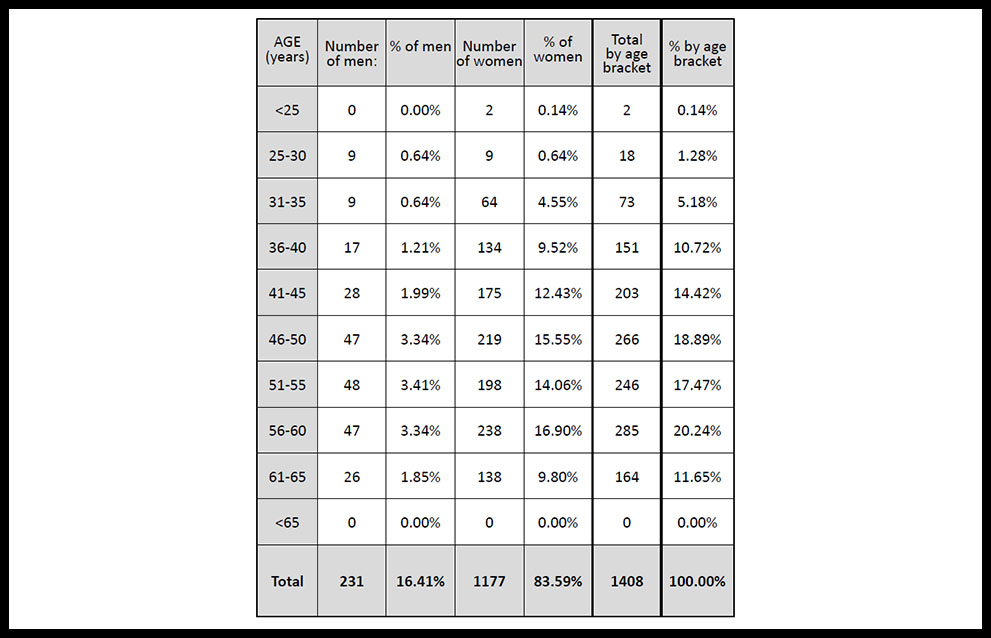
Table 2. Quantitative distribution of hospital nurses staff (nurses) by age and sex.
Figure 2 shows the working nursing population pyramid for the hospital studied. The progressive increase up to the 46 to 50 age bracket stands out, with a drop off that is seen again in the final 61-65 bracket and the absence of nurses aged over 65. It is striking that the narrowing of the 51-55 age bracket is solely at the expense of women. Female nurses dominate in the 56 to 60 bracket, while men dominate the 51 to 55 bracket and figures for both sexes lower in the final age bracket (61 to 65) lower than in the immediately preceding bracket (56 to 60). The negligible 0.14% of nurses aged under 25 is also striking.
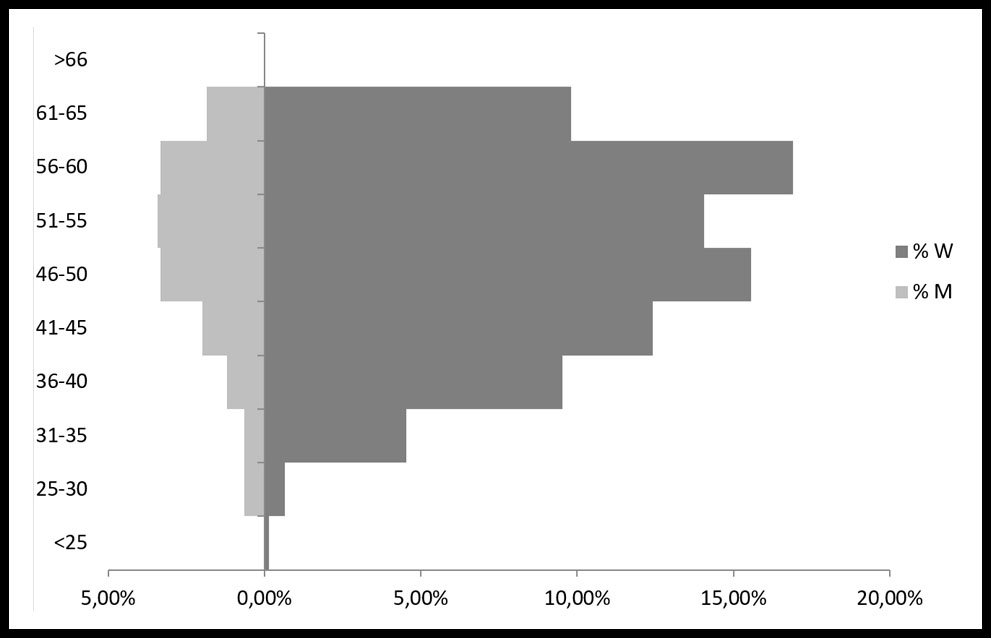
Figure 2. Nurses population pyramid according to age and sex from a southern Spain regional hospital.
Observing the evolution of the working population of the hospital over the last decade is also part of the main objective. To do so we have compared the data obtained in 2017 with those published in the 2006 annual report of the same hospital. According to the 2006 report, female nursing staff was also predominant at 27.72% followed by nursing assistant staff (20.54%), hospitality, laundry, services and social assistance (15.88%), physicians (12.37%), administrative staff (9.02%), junior physicians (6.17%), technical specialists (4.62%), maintenance professionals (2.99%), coordinators (0.26%) and managers (0.42%). Table 3 compares the total population of the hospital staff reflected in the 2006 annual reports with the data obtained in 2007, grouped by age bracket and sex. The 41 to 50 age bracket is the most predominant in the 2006 report while in 2017 it is the 51 to 60 bracket. We observe in both sexes a progression in terms of the predominant age brackets towards older age brackets; after a decade the working population over 50 (57.16%) has already overtaking those under 50 despite the numbers in the age bracket from 50 to retirement age being lower. In the 2006 report, of the 5,043 persons making up the working population, less than a third (30.85%) were over 50. In the 2006 report, 4 nurses retired past 65. Not one did so according to the data registered in 2017.
With respect to sex, the percentage of women has increased in the total population of the hospital over the last decade, going from 70.37% in the 2006 report to 73.47% in 2017.
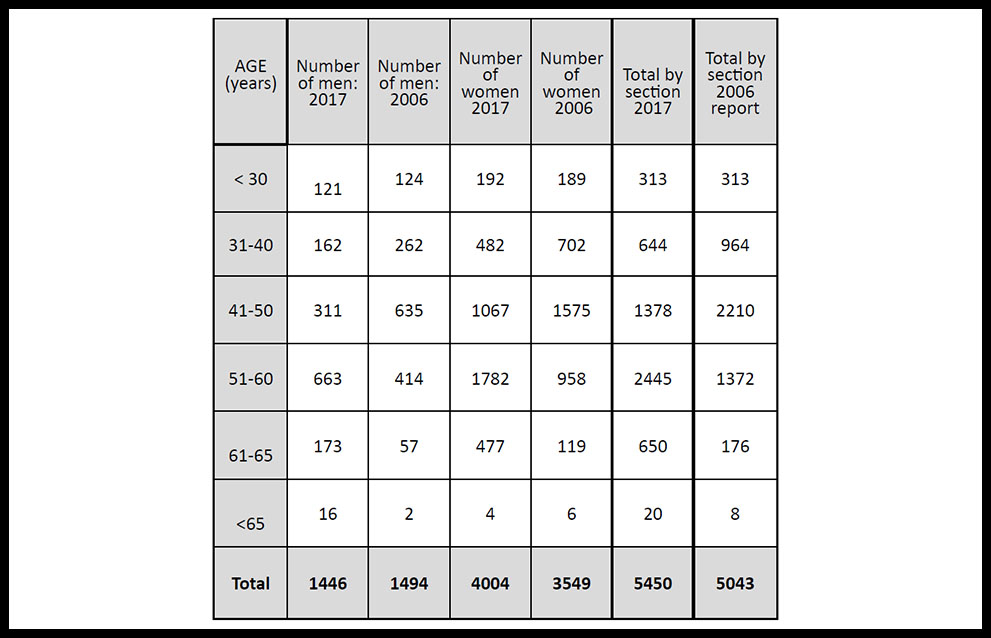
Table 3. Comparison by age brackets of the total hospital population in 2017 with the publication of the 2006 report.
DISCUSSION
The working population pyramid obtained is a reflection of the contemporary demographic situation in the general Spanish population (2), reaffirming the forecasts for 2025 in Andalusia (10). The ageing of the hospital’s staff is an example of what is happening on the international level (11). Facts such as the decrease in birth and mortality rates in the working population may have influenced this ageing, along with other factors, among them the adjustment measures taking during the recent recession. The Spanish Administration, where healthcare and education account for the majority of the 3.3 million public employees, saw the number of public servants over 60 surpass the number of those aged under 30 in 2016 (12). Thus, 17% of the working population of Spain are employed in the public sector, compared to 21% in the OECD, with more than half the public service belonging to the country’s autonomous communities (12).
The working population pyramid obtained reveals the low percentage of young people. The increase shown in the results for the 25 to 30 age bracket in the total population of the hospital is basically due to the contracting of junior specialist physician staff who predominantly come under this age bracket (13). In contrast with the low percentage of nurses among the younger population, a notable situation, as a “snapshot” of what might be occurring in the hospitals of the Spanish National Health System. The reality is that the main access route of new nursing graduates to join the National Health System is the specialist internal resident exam. It is a significant challenge considering the low number of places offered and the high number of nursing graduates who present for the annual national examination. Moreover, the duration of the residency for nursing specialists (just two years) and the lack of correlation between the working and category and the actual specialisation in the majority of cases makes workplace insertion very difficult for young specialist nurses in National Health System hospitals (14). Many of them are forced to emigrate to other countries which then benefit from their experience and the cost of their training, reinforcing the ageing of the population at home further. It is even more ironic as an ageing population requires more and better nursing care.
Other factors may have influenced the drop of in the 31 to 35 age bracket. Among them the temporary nature of the current access contracts and systems to Spanish public service which generally penalise young people with lower seniority. It would seem desirable that with an ageing working population, measures would be introduced to allow for greater flexibility of access. In particular in relation to those centres with lower National Health System demand (local hospitals, rural health centres, etc.).
On the other hand, the narrowing of the 61 to 65 age bracket indicates that a percentage of hospital staff do not retire at the legal age of 65 in Spain. No nurse did so over 65. One must ask the reasons why staff in general and nurses in particular retire early. The literature suggests that capacity to work is affected as staff grows older (15) with older people needing longer periods to recover from health problems than young people (15). The majority of nurses claim to be most affected by musculoskeletal conditions (11,17,18) pathologies which begin to emerge in their 40s and 50s (11).
In terms of sex, the pyramid is asymmetrical with clear female predominance in the hospital population, which is even more pronounced in nursing. Almost three quarters of the staff are women, as are almost 84% of all nurses. Furthermore, female predominance in the working population of the hospital has increased compared to the data in the 2006 report.
As the saying goes, one can’t see the wood for the trees. The data obtained in the nursing population pyramid might also reveal a practical application for the early detection of possible damage on a collective level in terms of sex. Specifically, the drop off of female nurses in the 51 to 55 age bracket is notable. Given that this does not occur with male nurses nor for the total hospital population in the same age bracket, it interrupts the progressive growth of the working population in the age brackets immediately below (figure 2). Its detection obliges us to plan the monitoring of individual health, including the application of a capacity to work survey (19), and adequate monitoring of nurses in this age bracket. It would also force us to engage in the necessary coordination with the Human Resources department to analyse the situation and pinpoint the causes in order to propose preventive and corrective measures. Several circumstances might be involved in the narrowing of age brackets detected. On the one hand, it may be due to internal mobility in the health systems, such as the transfer of specialised services (hospitals) to primary care (health centres) periodic mobility tenders. It would be useful, therefore, to compare the primary care nursing population pyramid for the same city. On the other hand, it may be influenced by temporary incapacity processes due to certain pathologies that would cause departure from the company. It would be necessary to also analyse the working conditions and other factors, including the dual presence of female nurses (20), caring for other people in the family environment or other aspects such as shifts. Unlike physicians, who enjoy the privilege of choosing to opt out of night shifts from the age of 55, this is more complicated for nursing staff. Some studies show that the impact of sustained night shifts on nurses’ health (21). In the literature (17,18,22) we can find the reasons the lead to the early retirement of nurses. Among them are rotating shifts and night shifts which alter their circadian rhythms, restricting their time for personal life. There is also mention of physical problems, a lack of time to attend to family tasks, the use of new technologies, feeling under-appreciated (both economically and socially) in spite of the experience they possess or feeling discriminated against based on ageist stereotypes. Indeed, various authors (23-27) suggest measures to prevent early retirement. Among them are better recognition for experience after years of work, avoiding stereotypes and prejudice; ergonomic improvements to facilitate the work of nurses (for example, larger screens for better visualization); sharing work, redesigning working methods to reduce workload; shorter shifts; flexible organisation; training courses for older nurses (both in new technologies and any other area, with the same conditions as for younger nurses), or progressive dedication to training to transfer their knowledge and experience to new generations. With respect to night shifts, it would be reasonable to allow nurses aged over 55 to opt out from this age, as is the case for physicians, and that these shifts are progressively assumed by younger nurses. This would reduce the excessive load on ageing staff, mitigating the social, health and economic consequences in terms of damage to the maintenance of the welfare state.
One limitation of the study may be the number of staff with temporary contracts at the time of the study (January) compared to other times of year such as the summer months. On the other hand, we believe that the strength of the utility that studies such as this may have as an instrument for the monitoring of collective health, and the implications for shaping health policies and management by taking into account how the working population is progressing in the health system with a view to implementing the necessary measures.
CONCLUSIONS
In conclusion, the study carried out in a referral hospital shows a working population that has aged and has been further feminised over the last decade, especially in nursing. The shift towards older age brackets a decade on is striking, with the working population over 50 constituting more than 50% of the personnel, with the average age of the working population at the centre having also increased. Within the nursing population, the narrowing of the 51 to 55 age bracket is also striking, the lack of young staff and an ever increasing fall off in the age bracket of retirement age. These are facts which must draw the attention of managers to put in place realistic and efficient measures that promote the “active ageing” so often spoken of as well as others that facilitate the entry into the labour market of young nurses, especially in a country, Spain, with such a high rate of youth unemployment.
BIBLIOGRAPHY
- Institute of Sciences and Polymer Technology Anuario estadístico de Andalucía. [consulted on 31/10/2018]. Available at: http://www.juntadeandalucia.es/institutodeestadisticaycartografia/anuario/index.htm
- Instituto Nacional de Estadística. [consulted on 31/10/2018]. Available at: https://www.ine.es/censos2011_datos/cen11_datos_inicio.htm
- Eurostat. Your key to European Statistics. [consulted on 31/10/2018]. Available at: https://ec.europa.eu/eurostat
- Rechel B, Grundy E, Robine JM, et al. Ageing in the European Union. The Lancet. 2013;381:1312-22.
- Abades Porcel M, Rayón Valpuesta E. El envejecimiento en España: ¿un reto o un problema social?. Gerokomos. 2012;23:151-5.
- Real Decreto por el que se establecen los criterios básicos sobre la organización de recursos para desarrollar la actividad sanitaria de los servicios de prevención. RD Nº 843/2011 (4 June 2011).
- Urbaneja Arrue F, Lijó Bilbao A, Cabrerizo Benito JI, et al. Vigilancia epidemiológica en el trabajo. Guía para la implantación de la vigilancia de la salud por parte de los servicios de prevención. Barakaldo: OSALAN; 2015. 131 p.
- Aranda Lara JM. Informe anual 2006. Tomo I. Actividad General. Hospital Universitario Reina Sofía; 2006.
- Acuerdo de la comisión de recursos humanos del Sistema Nacional de Salud, por el que se aprueba el protocolo mediante el que se determinan pautas básicas destinadas a asegurar y proteger el derecho a la intimidad del paciente por los alumnos y residentes en Ciencias de la Salud. OL Nº SSI/81/2017 (19 January 2017).
- Pirámide de población de Andalucía: Anuario Estadístico de Andalucía; [consulted on 31/10/2018]. Available at: http://www.juntadeandalucia.es/institutodeestadisticaycartografia/iea/consultasActividad.jsp?CodOper=64&sub=992
- Graham EM, Duffield C. An ageing nursing workforce. Australian Health Review. 2010;34:44–8.
- Losada Marrodan C, Alvareda Sanz A, Longo Martínez F, et al. El empleo público en España: desafíos para un estado democrático más eficaz. Madrid Instituto de Estudios Económicos; 2017. 215 p.
- Ranchal Sánchez A, Pérula De Torres LA, Santos Luna F, et al. Prevalence of tobacco consumption among Young physicians at a regional university hospital in southern Spain: a cross-sectional study. BMJ [electronic version]. 2018 [consulted on 01/11/2018]. Available at: https://bmjopen.bmj.com/content/8/2/e018728
- Ranchal A, Jolley MJ, Keogh J, Lepiesova M, Rasku T, Zeller S. The challenge of the standardization of nursing specializations in Europe. Int Nursing Rev. 2015. doi.org/10.1111/inr.12204.
- Monteiro MS, Alexandre NM, Milani D, et al. Work capacity evaluation among nursing aides. Rev Esc Enferm. 2011;45:1177-82.
- Keller SM, Burns CM. The aging nurse. AAOHN. 2010;58:437-44.
- Fragar LJ, Depczynski JC. Beyond 50. Challenges at work for older nurses and allied health workers in rural Australia: a thematic analysis of focus group discussions. BMC Health Serv Res. 2011;21:11:42.
- Uthaman T, Chua TL, Ang SY. Older nurses: A literature review on challenges, factors in early retirement and workforce retention. Proceedings of Singapore Healthcare.2015;25:50–5.
- Ilmarinen J. The work ability index (WAI). Occup med. 2007;57(2):160.
- Zito M, Colombo L, Mura G. Job demands and work-family conflict in a health care staff. The role of work shifts. G Ital Med Lav Ergon. 2013;35(3):168-175.
- Yuan X, Zhu C, Wang M, et al. Night Shift Work Increases the Risks of Multiple Primary Cancers in Women: A Systematic Review and Meta-analysis of 61 Articles. Cancer Epidemiol Biomarkers Prev. 2018;27(1):25-40.
- Walker L, Clendon J. Early nurse attrition in New Zealand associated policy implications. Int Nurs Rev. 2018;65(1):33-40.
- Cohen JD. The aging nursing workforce: How to retain experienced nurses. J Healthc Manag. 2006;51(4):233-45
- Stichler JF. Healthy work environments for the ageing nursing workforce. J Nurs Manag. 2013;21(7):956-63.
- Graham E, Donoghue J, Duffield Ch. Why Do Older RNs Keep Working?. JONA. 2014;44(11):591-7.
- Cyr JP. Retaining older hospital nurses and delaying their retirement. J Nurs Adm. 2005;35(12):563-7.
- Mion LC, Hazel C, Cap M, et al. Retaining and recruiting mature experienced nurses: a multicomponent organizational strategy. J Nurs Adm. 2006;36(3):148-54.
ARTICLE INFORMATION
Corresponding Author: Antonio Ranchal Sánchez. Facultad de Medicina y Enfermería, Edificio Sur. Avda. Menéndez Pidal s/n. Córdoba 14004. Correo electrónico: en1rasaa@uco.es





