














 154 / 64
154 / 64

154
Ismael Khouly, DDS, MS, PhD
Treatment Options for the Atrophic Posterior Maxilla
A modified transcrestal approach with a vertical slot
osteotomy (OASA technique) was proposed to provide good
visual access in order to reflect the Schneiderian membrane
at the inferior border of the sinus floor, avoid perforation of
membrane, obtain access to repair membrane perforation,
and have control of bone graft placement.(15) Drilling with
direct vision and protection of the membrane avoided the
trauma of the osteotome touching the membrane, which also
decreased the chances of perforation related to the tapping
sequence.(31,32) However, this procedure may increase time
and morbidity to the patient. (15)
Currently, which bone graft material is most effective for
these techniques is unknown. A number of clinical studies using
a variety of autogenous bone grafts, allografts, xenografts, and
alloplast in the posterior maxilla have been conducted and
were discussed in a number of systematic reviews. (5-8,33-
37) As described in the literature, such heterogeneity had no
relevant effect on the clinical outcomes. (38,39) Although, sinus
augmentation without graft have been reported successfully
using lateral wall or osteotome procedures. (40,41) Moreover,
no significant difference in outcomes were reported between
studies using bone graft materials during sinus augmentation
versus no graft material. (26) The surgical concern is how to
achieve better blood supply and better stability for placed
implants, while avoiding trauma.
Recently, short implants (less than 10 mm long) have been
proposed as an alternative to sinus augmentation in order to
rehabilitate posterior maxilla. (13,14) The use of short implants
may reduce the occurrence of surgical complications and
avoid augmentation procedures reducing patient’s discomfort.
(13,14,42) Prior to placement of short implants the residual
bone height and width must be evaluated carefully. There
must be sufficient residual volume to accommodate the
implants ensuring primary stability. The use of short implants is
promising but needs further investigation to be considered as
effective as the other techniques in the long term. (43)
A careful evaluation of the sinus anatomy is mandatory
prior to any surgical procedure involving the sinus. Studies
by Avila et al (44) and Soardi et al (45) reported that a direct
relation exists between sinus morphology and vital bone
formation. The results of these studies demonstrated that
sinuses with a narrow horizontal width and greater exposure
of the medial and lateral walls showed a greater percentage of
vital bone than sinuses with a wider width and less surrounding
bone exposure. They showed that significant time is necessary
for graft maturation, especially in wide sinuses. Since the blood
supply to the sinus is critical for healing and bone formation
any factor that brings this supply closer to the graft material
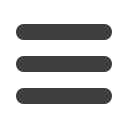
would be expected to improve healing. For example, a sinus
with a narrow horizontal width, closer proximity of surrounding
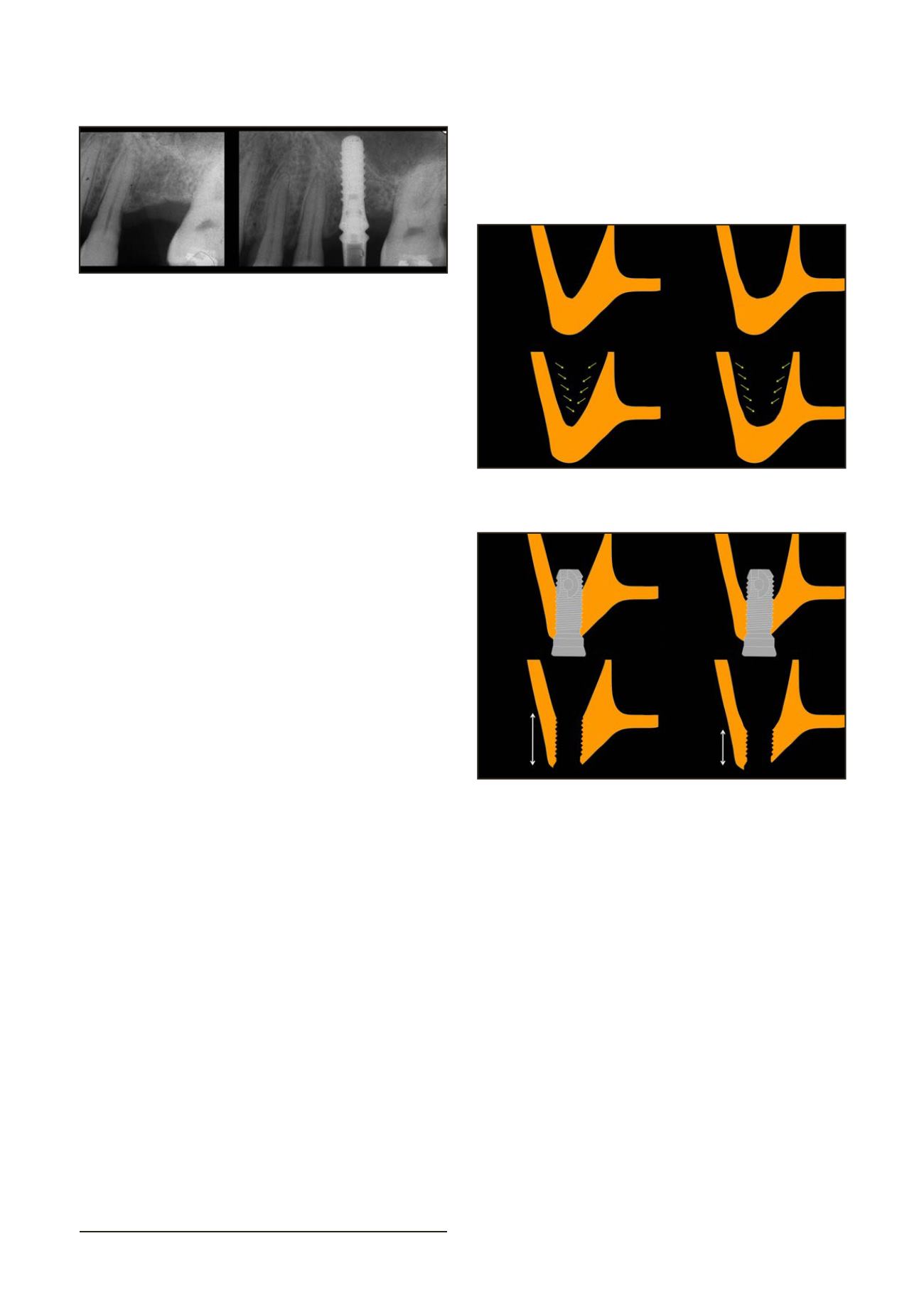
walls, and V-shaped allows better blood supply and better
stability when implants are placed simultaneously. (Fig. 4, 5)
The implants will support the Schneiderian membrane and
the site can heal even without adding bone grafting. In narrow
maxillary sinuses, the higher amount of remaining residual
crestal bone and presence of slope, the osteotome procedures
may be recommended. A smaller width and height would allow
cells and healing proteins less distance to migrate. However,
wide, U-shaped sinuses may provide less chances of blood
supply. For cases with less of crestal bone and a flatter sinus
floor in wide sinus, a conventional sinus augmentation with
lateral wall procedure may provide more predictable outcomes.
CONCLUSIONS
The primary purpose of sinus lift procedure is to create
sufficient bone structure to allow implant placement and its
posterior prostheses in a predictable way. Which technique to
use depends on the ability and experience of the operator and
the anatomical characteristics of the remaining bone. Based on
the remaining bone, the following guidelines are suggested: with
a residual bone height (RBH) of 4mm or less, a LWSFE procedure
is recommended for single or multiple implant placement; with
4-7mm of RBH, a OASA technique is recommended for single
implants and a LWSFE for multiple implant placement; with more
than 7mm of RBH, BAOSFE can be used. Simultaneous implant
placement is recommended whenever primary stability can be
obtained, this occurs more often in V-shaped sinuses.
Using the proposed guidelines, careful case and material
selection corresponding to different indications can be beneficial
to achieve predictable treatment outcomes in the posterior
atrophic maxilla. Even though sinus lift procedures have been
thoroughly studied for several years, further studies including
sinus anatomy should assess improvements in this field.
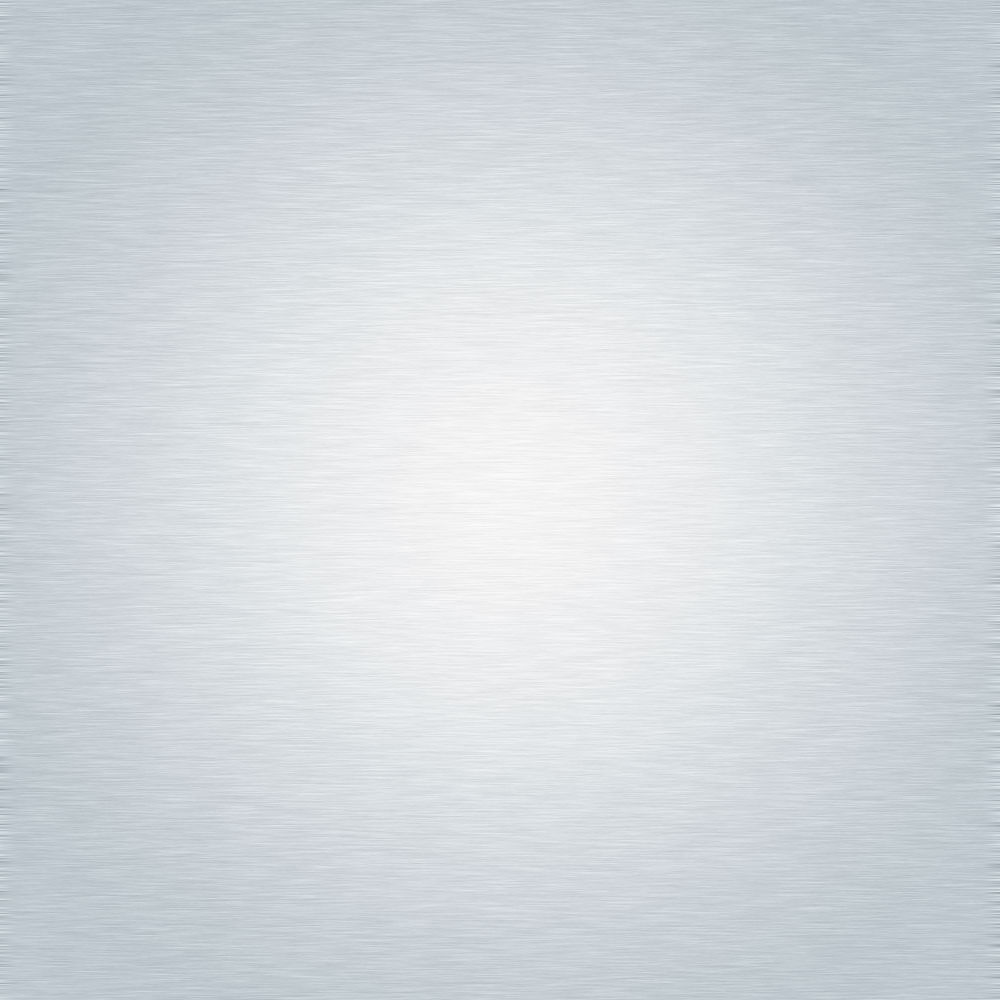
Figure 3. Periapical X-Rays of implant placed using BAOSFE
technique, prior to surgery and 6 months post-surgery.
Figure 4. Relation between sinus morphology and vital bone
formation.
Figure 5. Implant stabilization regarding the sinus shape (V-shaped
vs U-shaped)