43
Otoneurología 2014:
comprendiendomejor los trastornos vestibulares
SUPLEMENTO
original
Actual.Med.
2014; 99: (791). Supl. 43-60
representing a proportion of 2,1%; 313 (12% of the sample) were
cataloguedasUVH,and2239 (85,9%)completedtheNPVHgroup.
Given the population attended in our department
(approximately 350000 inhabitants) and according to this data, an
estimated prevalence of 15,7 cases per 100000 can be inferred for
bilateral vestibularhypofunction inour area, but thisestimationmay
have little if not none value, as, in spite that it is impossible for us to
obtain theexactdata,weassume that thesepatientsarenot referred
toourunit inaquitesignificantproportion.
Among the BVH group, 56,4% were female patients, which
was similar to the proportion found in theUVH group (58,5%), and
statisticallysignificantly less(p=0,03)than intheNPVH,wherea65,1%
of femalepatientswas found.
Agewassignificantlyhigher in theBVHgroup than in the restof
thegroups (mean61,04,compared to52,56amongUVHand52,81 in
theNPVH),givingap=0,004 fortheKruskal-Wallistest.
Wardet al (1), reviewed21782adult respondent toaNational
Health surveycarriedout inUS, and foundaestimatedprevalenceof
BVHof 28per 100000adults,which isnearly twiceasmuchaswhat
weestimatedarisingfromourpatients.Thereasonsforthisdifference
must be looked for, in one hand, in the definition of case, which
was based on the symptoms ticked in the survey described in the
referencedpaper, but linked strictly to the caloric test inour analysis.
On theotherhand, as itwasmentionedbefore, anotminor amount
of patientswithBVHmight beoverlooked, or simply not referred in
ourarea.
IncidenceofBVHhasbeenestimatedas1,7patientsper100000
adults (2)which is roughlyhalf asmuchas thatof themost common
cause of UVH (vestibular neuritis) (3). However, only 2% of the
patientsevaluated inourvestibularclinicwasdiagnosedofBVH,while
vestibularneuritiswasfound in8%ofpatients,givinganotherexample
of theattributedmisdiagnosisofBVH, thatcouldmakeGPorENT less
pronetoreferthesepatients.
Kimetal(4)observedaslightfemalepreponderanceforBVH,but
the referral patternsmayact asabias in thisparticular aspect. Inour
case, theresultsarecoincident.Thegroupwithahigherproportionof
femalepatientswasNPVH, includingBVHandUVHbothasimilarrate
male:female.
Meanageof BVH inour studiowas similar towhat isexpected
accordingtothe literature (5)
ETIOLOGY
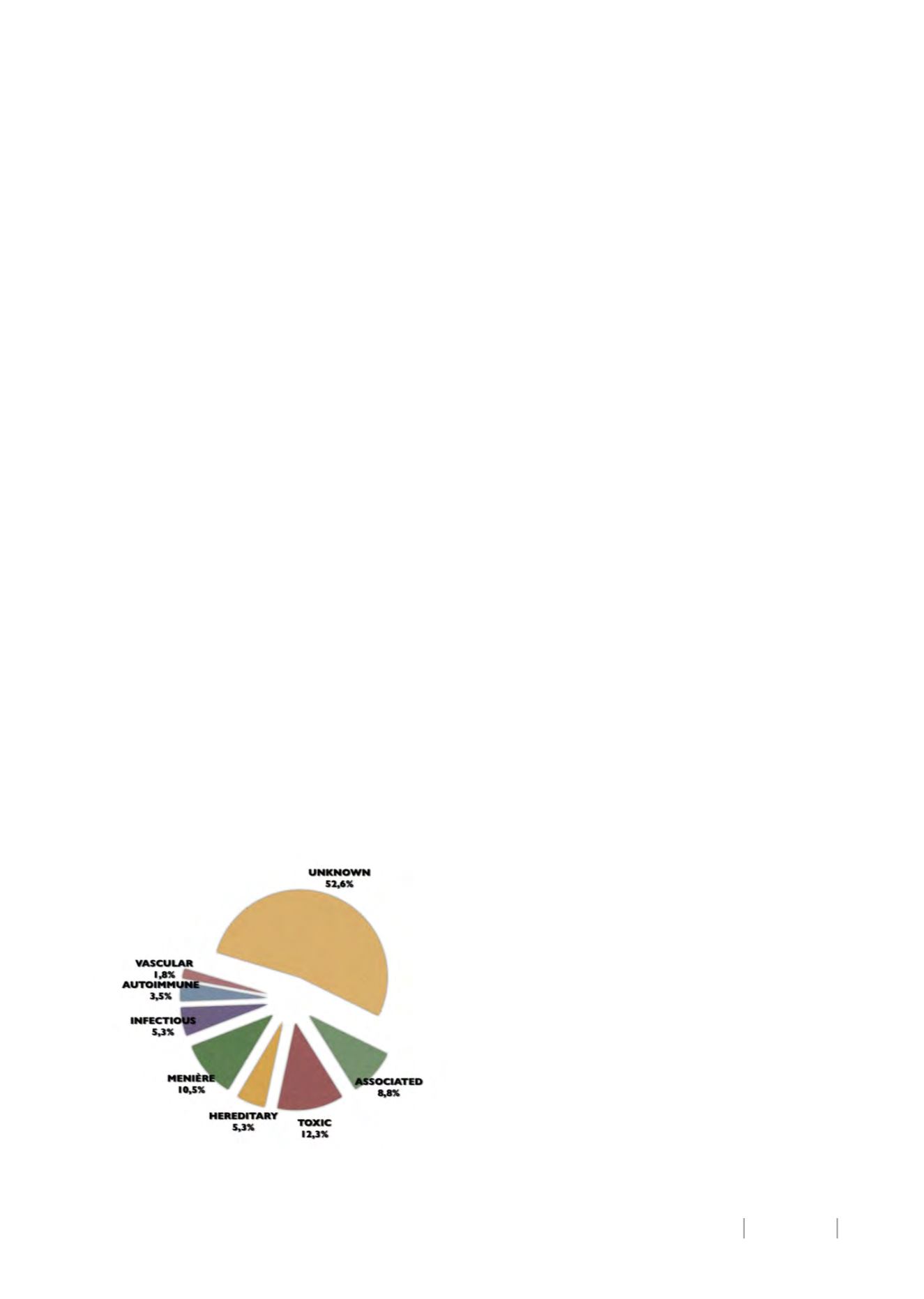
As demonstrated infigure1,wedidnot finda cause for the
BVH in a 52,6% of patients. Most frequent known causes were
toxic (12,3%),Menière’s disease (10,5%) and infectious (5,3%).
Figure1. CausesofBVH found inour studypopulation.
Zingler et al (3) reviewed 255 cases of BVH, finding that
themost common causeswereototoxicaminoglycosides (13%),
Menière’s disease (7%), andmeningitis (5%). Thedefinite cause
of BVHwas determined in 24% and the probable cause in 25%
havinghalf of thepatients anot known cause for their problem.
Rinne et al (6) also found gentamicin ototoxicity in a 17%,
while autoimmune disease was present in 9% of patients and
otological or neoplastic disease in the 13% of patients. In this
studio, it was concluded that neurological, audiological and
ocular motor assessments allow the probable cause of BVH to
be defined in approximately 80% of cases. Idiopatic BVHwould
be certificated in a21%of thepatients.
Both papers describe a not minor proportion of patients
with associated neurological impairment (specially cerebellar
signs),whichwas reproducedas forour study representing8,8%
of patients. Among this group, we found a case of superficial
siderosis, a rare but described cause of BVH consisting on iron
deposition around the brain, brainstem and cerebellum that
associates progressivehearing and vestibular loss (7).
Zingler (4) found, regarding neurological comorbidities,
that cerebellar dysfunction was associated with peripheral
polyneuropathy in 32% compared with 18% in BVH patients
without cerebellar signs.
Other causes that must be taken into account are some
hereditaryhearing loss(DFNA9)syndromes(8),andheadtrauma(9).
SYMPTOMS
John Crawford (10) related, back in 1952, the somewhat
pitiful feeling of oscillopsia and imbalance that he experienced
after a streptomycin treatment for a suspected tuberculosis
arthritis. His essay, included in the forthcoming book “When
DoctorsArePatients”editedbyMaxPinner,M.D., andBenjamin
F. Miller, M.D., and published in 1952 by W. W. Norton and
Company (11), described perfectly the same example that we
use today to explain these symptoms to our patient’s relatives.
He stated: “… even in this position the pulse beat in my head
became a noticeable motion disturbing my equilibrium. Most
of us have experimented with motion pictures at home. This
experiencecanbeused to illustrate thesensationsof thepatient
with damage to the vestibular apparatus. Imagine the results
of a sequence taken by pointing the camera straight ahead,
holding it against the chest andwalking at a normal pace down
a city street. When a sequence thus taken is viewed on the
screen, the street seems to careen crazily in all directions, faces
of approaching persons become blurred and unrecognizable,
and the viewer may even experience a feeling of dizziness or
nausea as hewatches”.
BVH greatly burdens readjustments in posture that are
requiredwhenmaking rapidmovements, creatingamovement-
related sensationof blurry vision, andmakingnearly impossible
the maintenance of balance if there is deprivation of other
sensory entries, such as when walking in the dark or over
uneven superficies.
Likewise, visual information can be misinterpreted, as
there is not vestibular function to confront it.Motionof objects
around implies a continuous effort to discriminate information
and makes movement (own or environmental) extremely
uncomfortable.
Thiscontinuousefforttounderstandvisualorproprioceptive
informationdemands anexcessive concentrationonbalance, so
the patient quite frequently complains of cognitive symptoms,
which are well described even when evaluating UVH, and
related to a sensory mismatch between disordered vestibular
input andother sensory signals of orientation (12, 13).
Patients with BVH usually do not have vertigo related
complains, as these symptoms are consequence of asymmetry
of vestibular function. This particular characteristic must be
kept in mind when interrogating a dizzy patient, as balance
problems and blurry vision might only appear when moving


