46
original
SUPLEMENTO
Otoneurología 2014:
comprendiendomejor los trastornos vestibulares
Actual.Med.
2014; 99: (791). Supl. 46-60
(29), but, aside the above-mentioned incapacity to stand still
over a rubber foamwhile performing a Romberg test, little does
posturography bring to BVH diagnosis. However, this technology
isof use for treatment and follow-upof thesepatients.
Most common results of BVH patients for these tests are
summed in table1.
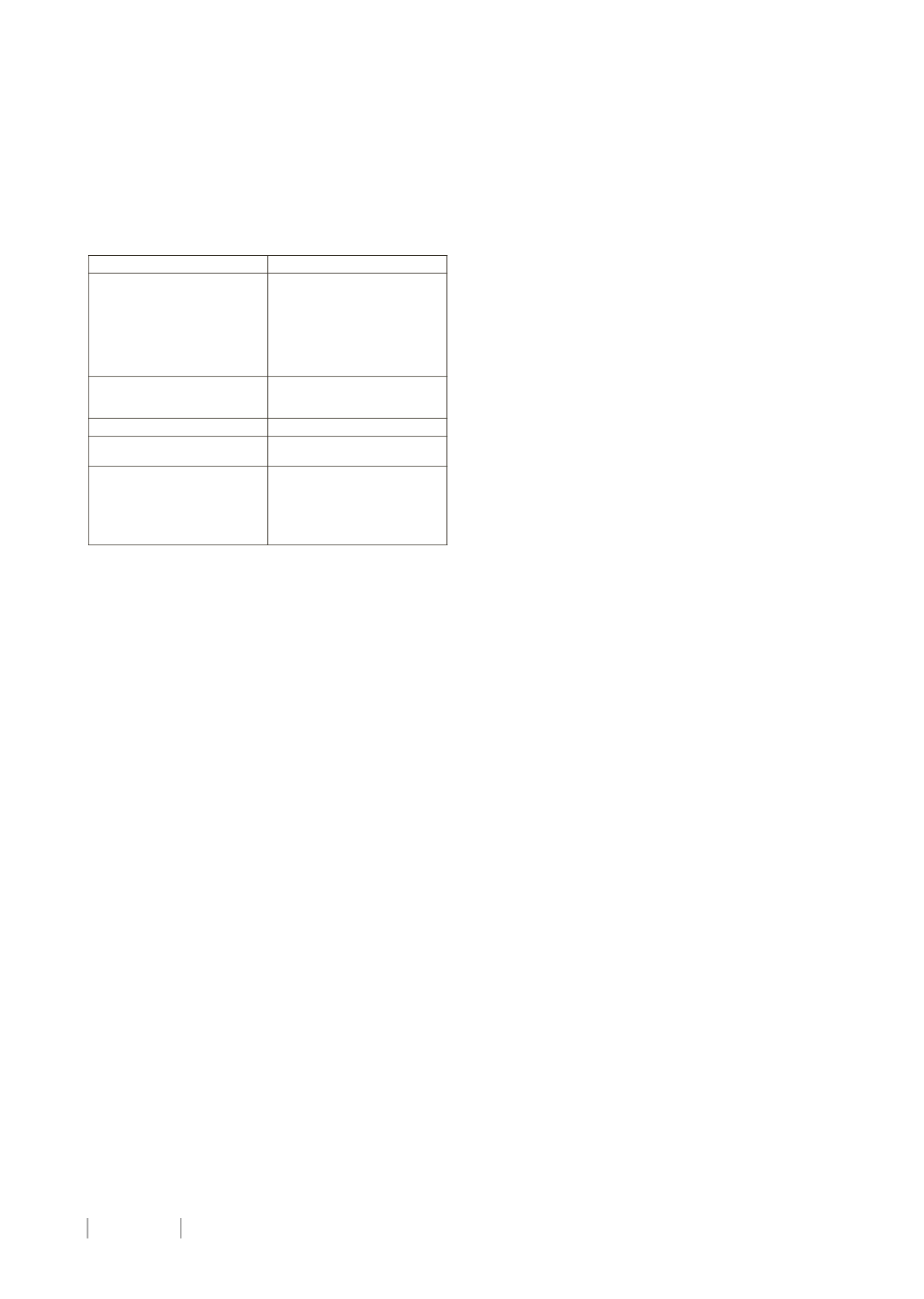
Table1. Typical BVH results incommonvestibular test
6.- Other tests.-
neuroimaging might be necessary in
situations such as head trauma and associated cerebellar
signs, supplemented, in particularly this last situation, with
neurophysiology tests (looking for peripheric neuropathy).
Likewise, laboratory tests (especiallyautoimmunebatteries) areof
use if infectiousor inflammatorydisease is suspected, andgenetic
assessment could be of help in cases of accompanying congenital
deafness or suspicion of hereditary ataxias (such as Friedrich or
SCA-3).
TREATMENT
Albeit specific treatments for autoimmune, neurological
or infectious possible etiologies, which are not addressed by
this review’s objectives, primary treatment for BVH is Vestibular
Rehabilitation (VR). Although it may be obvious, it is important
to stress the contraindication of vestibular suppressants for
all vestibular hypofunction (out of the acute arrest), and very
especiallywhen the impairment isbilateral.
Two main objectives must be pursued when rehabilitating
BVH: stabilizationof gaze, and stabilizationof gait.
Herdman (30) defined four mechanisms used to stabilize
gaze: change inamplitudeof saccades, useof corrective saccades,
modification of pursuit eyemovements, central preprogramming
of eyemovements. Thesemechanisms canbe addressed through
different exercises, such as focusing on a target while moving
head horizontally and vertically, pursuing a target that moves
alternately to both sides and vertically whilemoving head to the
oppositedirectionof the target (31),orperformingactiveeye-head
movementsbetween twohorizontal targets (30).
As for postural stability, exercises that train implementation
of proprioceptive and visual inputs are useful to progressively
regain control of gait. Some examples of these exercises can be
foundon the internet (32).
Patient isusuallyasked to repeatexercises3-5timeseachday
inthecaseofgazestabilizers,ortwiceeachday forposturalcontrol,
and supplement themwithdaily routines such aswalking at least
1 hour every day. Anyway, RV protocols must be tailored and
progressive, andalwaysadapted to thepatient’s clinical condition.
In our Neurotology unit, physical customized therapy is
prescribed following these principles, and supplemented with
posturography-based Rehabilitation, in order to reinforce the
learned new strategies with visual feedback and also store
comparablemilestonesofprogression.
Follow up andmeasurement of outcomes can be achieved
withposturography (as saidbefore),DVA,DHI and, nowespecially,
VHIT.
PROGNOSIS
There isenoughevidenceon theutilityofVR forUVH (33), and
use forothercausesofunsteadinesshasbeenalsoproposed (34,35).
However,whenevaluatingoutcomesofBVHpatients, Zingler
et al (5) found among their study population that only 29% of
patientssubjectivelyrated thecourseof theirdiseaseas improving.
Similar findings were related byWard et al (1), describing a
rather pessimistic sensation of their subjects about the course of
theirsymptoms.Bymean, theyhadconsulted5,6doctors,but75%
of patients stated that noneof themgave relief to their symptoms
and considered their disease to be stable or worsening along the
last12months.
Gillespie (36) reported a mediocre result of RV for BVH
patients, noticing improvementonlya51%of them.
There is, though, some favorable evidence that encourage
the use of RV for BVH patients. Krebs et al (37) concluded that
VR effectively improved functional, dynamic stability during
locomotion, but even strengthening exercises result in self-
reported symptomatic improvement.
Herdmanet al (38) stated that theuseof vestibular exercises
is the main factor involved in recovery of DVA in patients with
BVH, and theorized that exercisesmay foster the use of centrally
programmed eye movements that could substitute for the
vestibulo-ocular reflex.
Porciuncula et al (39) conducted a systematic review on
the effect of VR on adults with BVH, finding moderate evidence
strength on improved gaze and postural stability (ICF-Body
Functions) followingexercise-basedVR.
Currently, investigation is being carried out about an
implantable neuroelectronic vestibular prosthesis that emulates
the normal labyrinth by sensing headmovement andmodulating
activityonappropriatebranchesof thevestibularnerve (2).
In our study population, a statistically significant difference
was found between previous and post-treatment DHI (p=0,027
for Wilcoxon signed ranks test), and also when evaluating
improvement of DVA (p=0,005 forWilcoxon signed ranks test). In
fact, mean reduction of DVA impairment was significantly higher
in BVH group than in UVH group (p=0,022 for Mann Whitney’s
U test), as shown in figure 5. Nonetheless, subjective sensation
of patients and recovery of daily life activities despite treatment
remain evidently poorer among BVH (mean DHI 35,75) patients
than inUVH (meanDHI 20,72).
CONCLUSIONS
As can be inferred from the literature, BVH is amuchmore
complexproblemthanaminoglycosidetoxicity, thatcanandshould
be accurately diagnosed or, at least, suspected through thorough
interrogation and physical examination, even without assistant
technology.
Impact on daily life activities is extreme, and, although
outcome of RV is questionable, and, generally, poorer thanwhen
usedfor UVH treatment, improvement of gaze and gait stability
and, moreover, of handicap scores, is feasible and thus, should
be tried in order to improve quality of life for these otherwise
chronicallydizzypatients.
TEST
TYPICALRESULT
ROTARYCHAIRTEST
Reduced
gain.
Increased
phase. Cervico-ocular reflex
variably increased. Gain may be
normal or less decreased at the
beginning for high frequencies,
and can recover over time at
them (which is less probable for
low frequencies)
VIDEONYSTAGMOGRAPHY
Decreased response in all
irrigations. Couldbeno response
at all, even instilling icewater
VEMP
Attenuatedor no response
VIDEOHEAD IMPULSETEST
Decreased gain (bilaterally).
Overt and/or covert saccades
POSTUROGRAPHY
Increased overall score and
general poor performance. Fall
or greatly increased scores for
conditions removingordistorting
visual and/or proprioceptive
inputs


